


















")





Jane Green MBE says we’re living through the most exciting time for autism and neuroscience in education. In this article, she looks at hypermobility, and how the body shapes neurodivergence.
We are in a groundbreaking era of neuroscience for autism, ADHD, dyspraxia, and other neurodivergences. Research now confirms that connective tissue differences in neurodivergent people impact both physical and emotional health. Understanding this link can improve educational approaches, ensuring that physiological factors are considered alongside social and emotional support. If we fail to address the body’s role in neurodivergent experiences, we risk missing crucial opportunities to support students effectively, or improve attendance and attribute more to EBSA anxiety. We need a holistic view of neurodivergent education supported by those who know, can train and support. I was a missing student in education, dismissed as dim and a hypochondriac always. I left school early and only in later years after becoming a single parent of disabled children I learned to study. I did well but sadly had to medically retire as again not believed to be neurodivergent, I always knew I was different, or disabled and ill. I learnt to mask my pain, but masking pain invalidates your self worth. We cannot let it continue for the sake of future generations and long lasting mental trauma.
Hypermobility
Neuroscience research is revealing clear differences in the connective tissue of neurodivergent people. This tissue is weaker and stretchier than in the general population, leading to problems throughout the body, from joints and muscles to the digestive system. Many people think hypermobility is just about being extra flexible or doing party tricks with your joints, but it is much more. It affects the entire body, including brain connections. The formal terminology is complex, so we’ll use hypermobility as shorthand to refer to the real differences in the connective tissue which is found throughout the body. The effect is probably due to weaker collagen (a protein in the connective tissue) making the connective tissue weaker and stretchier than in the general population.
Sometimes this means that our tissues tear and our joints may dislocate. It can also have an effect on our organs and on the gastrointestinal tract from entry to exit. Hypermobility affects our eyes, ears, joints, muscles, breathing and autonomic nervous system. As the tissues are weaker, muscles have to work much, much harder to keep our bodies together. A formal diagnosis of hypermobility is rare for children under 18, but it can be called paediatric hypermobility spectrum disorder or generalised joint hypermobility. The most common test for hypermobility is the Beighton Score, though this test is less effective for those born male, who may still experience fatigue, migraines, stomach issues, constipation, and allergies like eczema, hay fever, and pseudoasthma. Among adults, hypermobile Ehlers-Danlos syndrome (hEDS) is the most common type of hypermobility.
Hypermobility and neurodivergence
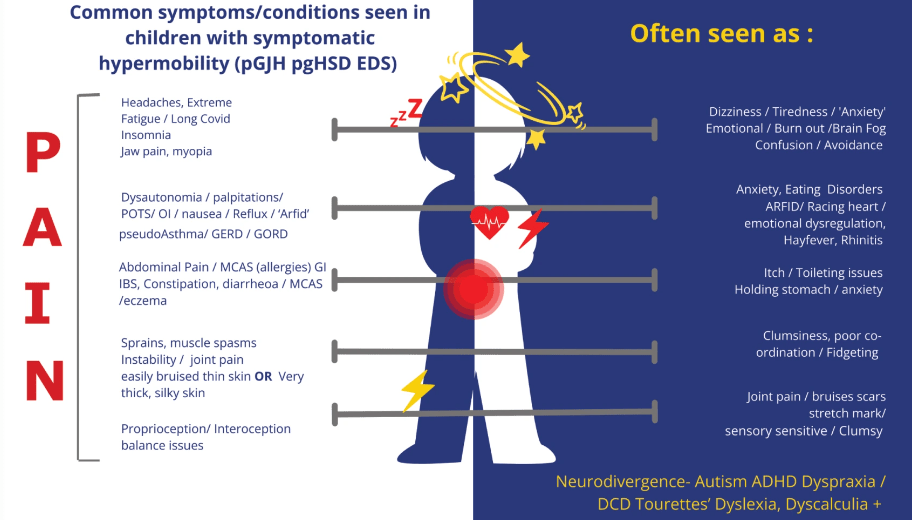
Autistic children and those with ADHD or dyspraxia often struggle at school because of social expectations and academic pressure. These demands can lead to burnout, fatigue, anxiety, and school avoidance. However, research suggests that internal physical factors may also play a role. Studies show that people with Ehlers-Danlos syndrome (EDS) are 74% more likely to be autistic and 56% more likely to have ADHD. A recent study found that neurodivergent individuals are more than twice as likely to have joint hypermobility, which increases pain and fatigue, so it’s their physical health conditions which are impacting school attendance and performance.
Common but often hidden symptoms include:
- Extreme tiredness
- Soft tissue and joint injuries
- Gastrointestinal issues affecting chewing, swallowing, digestion and bladder function
- Allergies
- Pain and anxiety
- Neurological issues like migraines, brain fog and confusion
- Dizziness, clumsiness and fainting
We rely on children to tell us when they are in pain, but a neurodivergent child may be hampered in communicating interoception (sensing internal stimuli within the body), proprioception (sensing position or movement of the body) and trauma from not being believed. Sadness and anger are examples of emotional displays for symptoms and subsequent symptomatic distress. For example, when a young person’s joints hurt, they may feel sad, frown or cry and as this pain turns to fatigue they may feel angry. In addition, behaviour can indicate symptom expression and distress including protective behaviours like rubbing the site of pain or self-injurious behaviours like self-scratching.
There’s a link between hypermobility, the brain and emotions
Because connective tissue supports blood circulation, a weaker structure means the heart has to work harder to pump oxygen to the brain. This can cause dizziness, brain fog, and confusion especially in autistic students and particularly girls from age 13 onwards. These symptoms are often mistaken for executive function difficulties, but the root cause is physiological. The body struggles to maintain blood flow, leading to increased heart rate, sweating, shallow breathing, and dizziness. To an outsider, this may look like social anxiety, but it is a physiological issue. If educational support focuses only on social-emotional mental health (SEMH) without addressing these physiological needs, outcomes will remain limited. The condition is often linked to dysfunctions in the autonomic nervous system, leading to disorders such as dysautonomia, orthostatic intolerance, and postural orthostatic tachycardia syndrome (POTS).
Proprioception, emotional regulation and hypermobility
It has been found that hypermobility affects proprioception, the body’s ability to sense its own position. Neurodivergent people with hypermobility often experience confusing or unexpected bodily sensations, making emotional regulation more difficult. When internal body signals are unclear, emotions can become harder to control, leading to anxiety and instability that is not just caused by external factors. Additionally, because the body works so hard to stay stable, individuals with hypermobility often need to move or fidget. Organ dysfunction, such as issues with digestion and bladder control, increases pain and inflammation, leading to extreme tiredness. Another study showed that students who appear clumsy and have proprioception issues may have brain fog and be more emotionally reactive.
Hypermobility and brain activity
Recent research using MRI scans explored how people with and without hypermobility react to emotions. When looking at different facial expressions, people with hypermobility and high anxiety had more activity in the amygdala (which detects threats) and the insular cortex (which processes internal body signals). The more severe their hypermobility, the harder these brain areas worked. This suggests that hypermobility is directly linked to emotional experiences and responses in the brain.
Further reading: Co-Occurring Physical Health Challenges in Neurodivergent Children and Young People: A Topical Review and Recommendation by Bethany Donaghy, David Moore and Jane Green
https://www.tandfonline.com/doi/full/10.1080/13575279.2022.2149471
Such an important article. These symptoms including the severe fatigue are real. We went to so many doctors who seemed to see only anxiety despite the fact there was never a day without pain. Thank you to SEDSConnective for helping to raise awareness!
Thanks so much for all your work Jane! Everything in this article describes my 8 year old son. He masked and tried his absolute hardest until a term into Year 2 and then no more…extreme burnout hit and we didn’t leave the house for months! We’re just rebuilding now, well over a year later. I doubt we’ll be able to return to the school system but thankfully Home Ed is well resourced in our area and we love the Self Directed Learning philosophy!